
What are Nitrates (Organic Nitrates)?
Nitrates (Organic Nitrates)
By Dr. Mahnoor Javed (Pharm D)
What are nitrates (organic nitrates): Nitrates (Organic nitrates), (and nitrites) used in the treatment of angina pectoris. They are simple nitric and nitrous acid esters of glycerol. They differ in their volatility. For example, isosorbide dinitrate and isosorbide mononitrate are solids at room temperature, nitroglycerin is only moderately volatile, and amyl nitrite is extremely volatile. These compounds cause a rapid reduction in myocardial oxygen demand, followed by rapid relief of symptoms. They are effective in stable and unstable angina as well as in variant angina pectoris
Organic Nitrates include:
Isosorbide dinitrate Dilatrate-SR, Isordil
Isosorbide mononitrate Imdur, Ismo
Nitroglycerin Nitro-BID, Nitro-Dur, Nitrolingual, Nitrostat
What is the Mechanism of Action of Nitrates (Organic Nitrates)?
Mechanism of Action:

Nitrates inhibit coronary vasoconstriction or spasm, increasing perfusion of the myocardium and, thus, relieving vasospastic angina. In addition, nitrates relax the veins (venodilation), decreasing preload and myocardial oxygen consumption. Because of this action, nitrates are effective in treating effort-induced angina (classic angina). Organic nitrates, such as nitroglycerin, which is also known as glyceryl trinitrate, are thought to relax vascular smooth muscle by their intracellular conversion to nitrite ions and then to nitric oxide, which, in turn, activates guanylate cyclase and increases the cells’ cyclic guanosine monophosphate (cGMP). Elevated cGMP ultimately leads to dephosphorylation of the myosin light chain, resulting in vascular smooth muscle relaxation.
What are the Effects of Nitrates (Organic Nitrates) on the cardiovascular system Cardiovascular Effects?
Hemodynamic Effects: Low concentrations of nitroglycerin preferentially dilate the veins more than the arterioles. This vasodilation decreases left and right ventricular chamber size and end-diastolic pressures but results in little change in systemic vascular resistance. Systemic arterial pressure may fall slightly, and heart rate is unchanged or may increase slightly in response to a decrease in blood pressure. Pulmonary vascular resistance and cardiac output are slightly reduced.
Doses of nitroglycerin that do not alter systemic arterial pressure often produce arteriolar dilation in the face and neck, resulting in a flush, or dilation of meningeal arterial vessels, causing headache. Higher doses of organic nitrates cause further venous pooling and also may decrease arteriolar resistance, thereby decreasing systolic and diastolic blood pressure and cardiac output and causing pallor, weakness, dizziness, and activation of compensatory sympathetic reflexes.
Coronary blood flow may increase transiently as a result of coronary vasodilation but may decrease subsequently if cardiac output and blood pressure decrease sufficiently.
In patients with autonomic dysfunction who cannot increase sympathetic outflow, the fall in blood pressure consequent to the venodilation produced by nitrates cannot be compensated; thus, nitrates may reduce arterial pressure and coronary perfusion pressure significantly, producing potentially life-threatening hypotension and even aggravating angina.
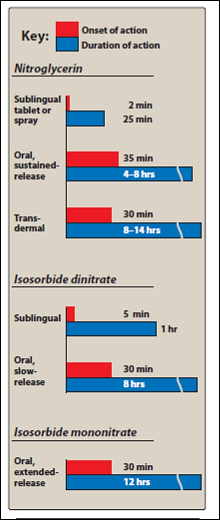
All of these agents are effective, but they differ in their onset of action and rate of elimination. For prompt relief of an ongoing attack of angina precipitated by exercise or emotional stress, sublingual (or spray form) nitroglycerin is the drug of choice.
At therapeutic doses, nitroglycerin has two major effects. First, it causes dilation of the large veins, resulting in pooling of blood in the veins. This diminishes preload (venous return to the heart) and reduces the work of the heart. Second, nitroglycerin dilates the coronary vasculature, providing an increased blood supply to the heart muscle. Nitroglycerin decreases myocardial oxygen consumption because of decreased cardiac work.
What are the Mechanism of Relief of Symptoms of Angina Pectoris by Nitrates (Organic Nitrates)?
Symptoms of Angina Pectoris:
The nitrate-induced relief of angina pain is through a decrease in cardiac work secondary to the fall in systemic arterial pressure.
High doses of organic nitrates may reduce blood pressure to such an extent that coronary flow is compromised; reflex tachycardia and adrenergic enhancement of contractility also occur. These effects may override the beneficial action of the drugs on myocardial oxygen demand and can aggravate ischemia. Additionally, sublingual nitroglycerin administration may produce bradycardia and hypotension.
What is the Interaction of Nitrates (Organic Nitrates) with (PDE5) Phosphodiesterase 5 Inhibitors?
Erectile dysfunction is a frequently encountered problem whose risk factors parallel those of coronary artery disease. Thus, many men desiring therapy for erectile dysfunction already may be receiving antianginal therapy.The phosphodiesterase 5 (PDE5) inhibitors sildenafil (VIAGRA), tadalafil (CIALIS), and vardenafil (LEVITRA) have been developed and widely used for therapy of erectile dysfunction. In the presence of a PDE5 inhibitor, nitrates cause profound increases in cyclic GMP and can dramatically reduce blood pressure.
Thus, all three PDE5 inhibitors are contraindicated in patients taking organic nitrate vasodilators, as indicated by a “black box” warning on product labeling. In the event that patients develop significant hypotension following combined administration of PDE5 inhibitor and nitrate, fluids and adrenergic receptor agonists, if needed, should be used for support.
What are the Therapeutic uses of Nitrates (Organic Nitrates) ?Therapeutic Uses:
- Angina
- Congestive Heart Failure
- Acute Myocardial Infarction
- Variant (Prinzmetal) Angina
What are the Pharmacokinetics of Nitrates (Organic Nitrates)?
Pharmacokinetics of Nitrates (Organic Nitrates):
In humans, peak concentrations of nitroglycerin are found in plasma within 4 minutes of sublingual administration; the drug has a t1/2 of 1–3 minutes. The onset of action of nitroglycerin may be even more rapid if it is delivered as a sublingual spray. Anginal pain may be prevented when the drug is used prophylactically immediately prior to exercise or stress. The smallest effective dose should be prescribed. Patients should be instructed to seek medical attention immediately if three tablets taken over a 15-minute period do not relieve a sustained attack because this situation may be indicative of myocardial infarction or another cause of the pain.
Application of nitroglycerin ointment (2%) applied to the skin can relieve angina, prolong exercise capacity, and reduce ischemic ST-segment depression with exercise for 4 hours or more. Effects are apparent within 30–60 minutes (although absorption is variable) and last for 4–6 hours. The ointment is particularly useful for controlling nocturnal angina, which commonly develops within 3 hours after the patient goes to sleep.
Transdermal nitroglycerin disks use a nitroglycerin impregnated polymer that permits gradual absorption and a continuous plasma nitrate concentration over 24 hours. The onset of action is slow, with peak effects occurring at 1–2 hours. To avoid tolerance, therapy should be interrupted for at least 8 hours each day. With this regimen, long-term prophylaxis of ischemic episodes often can be attained.
Transmucosal or buccal nitroglycerin is inserted under the upper lip above the incisors, where it adheres to the gingiva and dissolves gradually in a uniform manner. Hemodynamic effects are seen within 2–5 minutes, and it is therefore useful for short-term prophylaxis of angina. Nitroglycerin continues to be released into the circulation for a prolonged period, and exercise tolerance may be enhanced for up to 5 hours.
Isosorbide Dinitrate (ISORDIL, SORBITRATE)
Sublingual administration produces maximal plasma concentrations of the drug by 6 minutes, and the fall in concentration is rapid (t1/2 of ~45 minutes). The major route of metabolism of isosorbide dinitrate in humans appears to be by enzymatic de-nitration followed by glucuronide conjugation. The primary initial metabolites, isosorbide-2-mononitrate and isosorbide-5-mononitrate, have longer half-lives (3–6 hours) and presumably contribute to therapeutic efficacy.
Isosorbide-5-Mononitrate (IMDUR)
This agent is available in tablet form. It does not undergo significant first-pass metabolism and so has excellent bioavailability after oral administration. The mononitrate has a significantly longer t1/2 than does isosorbide dinitrate and has been formulated as a plain tablet and as a sustained-release preparation; both have longer durations of action than the corresponding dosage forms of isosorbide dinitrate.
The time to onset of action varies from 1 minute for nitroglycerin to more than 1 hour for isosorbide mononitrate. Significant first-pass metabolism of nitroglycerin occurs in the liver. Therefore, it is common to take the drug either sublingually or via a transdermal patch, thereby avoiding this route of elimination. Isosorbide mononitrate owes its improved bioavailability and long duration of action to its stability against hepatic breakdown. Oral isosorbide dinitrate undergoes de-nitration to two mononitrates, both of which possess antianginal activity.
What are the Adverse effect of Nitrates (Organic Nitrates)?
Adverse effect of Nitrates (Organic Nitrates):
The most common adverse effect of nitroglycerin, as well as of the other nitrates, is headache. From 30 to 60 percent of patients receiving intermittent nitrate therapy with long-acting agents develop headaches. High doses of organic nitrates can also cause:
- Postural hypotension ( Orthostatic hypotension)
- Facial flushing and
- Tachycardia.
Phosphodiesterase V inhibitors such as sildenafil, tardenafil, and vardenafil potentiate the action of the nitrates. To preclude the dangerous hypotension that may occur, this combination is contraindicated.
What are the Tolerance of Nitrates (Organic Nitrates)
Tolerance of Nitrates (Organic Nitrates) :
Tolerance to the actions of nitrates develops rapidly. The blood vessels become desensitized to vasodilation. Tolerance can be overcome by providing a daily “nitrate-free interval” to restore sensitivity to the drug. This interval is typically 10 to 12 hours, usually at night, because demand on the heart is decreased at that time. Nitroglycerin patches are worn for 12 hours, then removed for 12 hours. However, variant angina worsens early in the morning, perhaps due to circadian catecholamine surges. Therefore, the nitrate-free interval in these patients should occur in the late afternoon. Patients who continue to have angina despite nitrate therapy may benefit from the addition of another class of agent.
REFERENCES:
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- lippincott’s pharmacology 5th edition
- Oxford Handbook of Clinical Pharmacy – Wiffen, Philip, Mitchell, Marc, Snelling, Melanie, Stoner,Nicola